
Disclosure: University of Michigan is an HP customer and has received loaned and/or donated equipment from HP.
XR projects can provide cost savings, increased access, and better feedback for users, transforming in-person trainings at medical centers and institutions at large.
Institutional Profile
One of the nation’s top public universities, the University of Michigan (U-M) has been a leader in research, learning, and teaching for more than 200 years. With the highest research volume of all public universities in the United States, U-M is advancing new solutions and knowledge in areas ranging from the COVID-19 pandemic to driverless vehicle technology, social justice, and carbon neutrality. Its main campus in Ann Arbor comprises 19 schools and colleges; there are also regional campuses in Dearborn and Flint and a nationally ranked health system, Michigan Medicine.
The Challenge/Opportunity
When a patient in a medical center experiences cardiac arrest, an interprofessional team of healthcare professionals come together to help, including doctors, nurses, respiratory therapists, and others. This group can sometimes include as many as fifteen people, and these professionals must work together to make quick decisions in a very intense environment with someone’s life on the line. A lot of skills are put to the test, and without training it can be difficult for medical teams to work together effectively to deliver the right treatment at the right time. “The problem isn’t the medicine. These healthcare professionals know the medicine. The problem is on the nontechnical side,” said Michael Cole, associate professor of emergency medicine at the University of Michigan Medical School (Michigan Medicine). The people in these situations are dealing with an incredibly high-stress and high-stakes environment that requires important cognitive and behavioral skills that are not typically emphasized in conventional healthcare curricula, skills such as situational awareness, leadership, and interprofessional communication.
In order to train personnel for the medical and nontechnical skills needed in these situations, medical centers typically send their healthcare professionals to simulation centers or purchase a medical training mannequin, which can cost upwards of $150,000. Cole was looking for options to replace this expensive and resource-intensive process, which requires learners to gather in the same location at the same time and requires a costly mannequin, a simulation center, and technical staff to run the event. After examining the potential outcomes and benefits, Cole believed that a virtual reality (VR) solution might offer a cheaper and more effective approach to training personnel for these high-stress situations. It’s much less expensive to purchase VR equipment and contract with a vendor to develop an application than to purchase the medical equipment and incur other expenses associated with running in-person simulations. Additionally, VR headsets increasingly include capabilities that can deepen the experience and expand the data collected. The Reverb G2 Omnicept Edition headset from HP, for example, provides a data stream on users’ attention, cognitive load, eye tracking, and other sensory information that can help provide more tailored feedback for trainers and trainees.
After conducting a needs assessment, the stated goal for this VR project was to “develop a multi-user, VR-based app that allows healthcare professionals to train in cardiac arrest care in a collaborative manner that provides them feedback on both their clinical decision-making skills as well as the cognitive and behavioral science—based skills necessary to optimally run a high-performance team.”
Process
Cole approached this challenge in a planned and collaborative manner, working internally with colleagues at Michigan Medicine, as well as collaborating with Jeremy Nelson, senior director of XR, Media Design & Production at the University of Michigan, and external vendors. Initially, Cole sought the current resources available at the institution to help identify the initial steps required to bring his VR cardiac arrest training simulation to life. He made efforts to have conversations—not just email threads—with the medical IT group, the main campus IT group, procurement, and the legal department. Those conversations led Cole to begin an official RFP process to help identify the right technology necessary for the training simulation, and during that process, Nelson and other IT professionals evaluated and recommended the most promising headsets. The in-person conversations also helped ensure project stakeholders were on the same page and following the relevant institutional policies. Throughout the process, Nelson was able to help bring essential expertise to the project and act as an advocate between Cole and the various stakeholders across and outside the institution. Cole and Nelson were able to create a multidisciplinary team that brought together essential skills across areas including medicine, analytics, vendor management, procurement, and business operations.
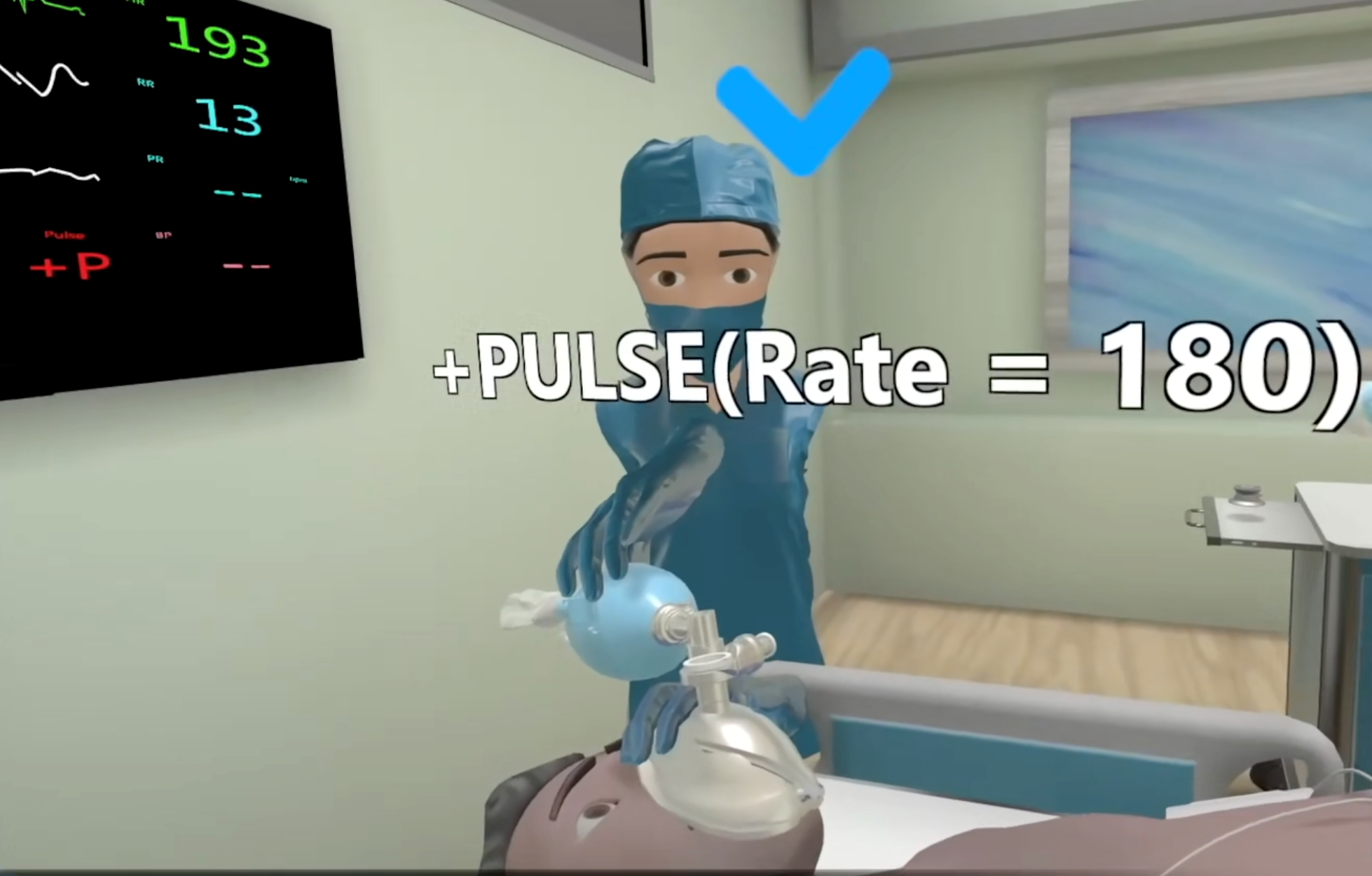
As part of the procurement process, Michigan staff interviewed several potential vendors for the creation of the two necessary aspects of their VR setup: the actual application that users would interact with in VR, and the processing of the attentional/cognitive load data based on the sensory output from the HP Omnicept headsets, which the team had chosen for this project. The sensors provide data on eye gaze and pupillary size, as well as heart rate and heart rate variability, all aspects that are much more difficult or impossible to track in a traditional training setting (see figure 1). The sensory output allows for reporting statistics not just on the cognitive load the headset already measures but also millisecond-by-millisecond statistics on where the users’ attention is during the simulated training experience and their natural responses to that experience. The app and the analytics aspects required Cole and Nelson to work with various IT stakeholders on campus to manage challenges such as data privacy, security, and headset approval. According to Cole, one of the most valuable groups of people he worked with during this project was a subgroup in IT focused on educational research: “These people were willing to understand the innovative nature of these activities and work with us instead of just saying no.” This group provides a network reserved to connect only preliminary devices for between six months and a year before they’ve gained full IT approval, which helps staff and faculty like Cole to both test and showcase their projects, reducing the wait time as they are being developed and approved.
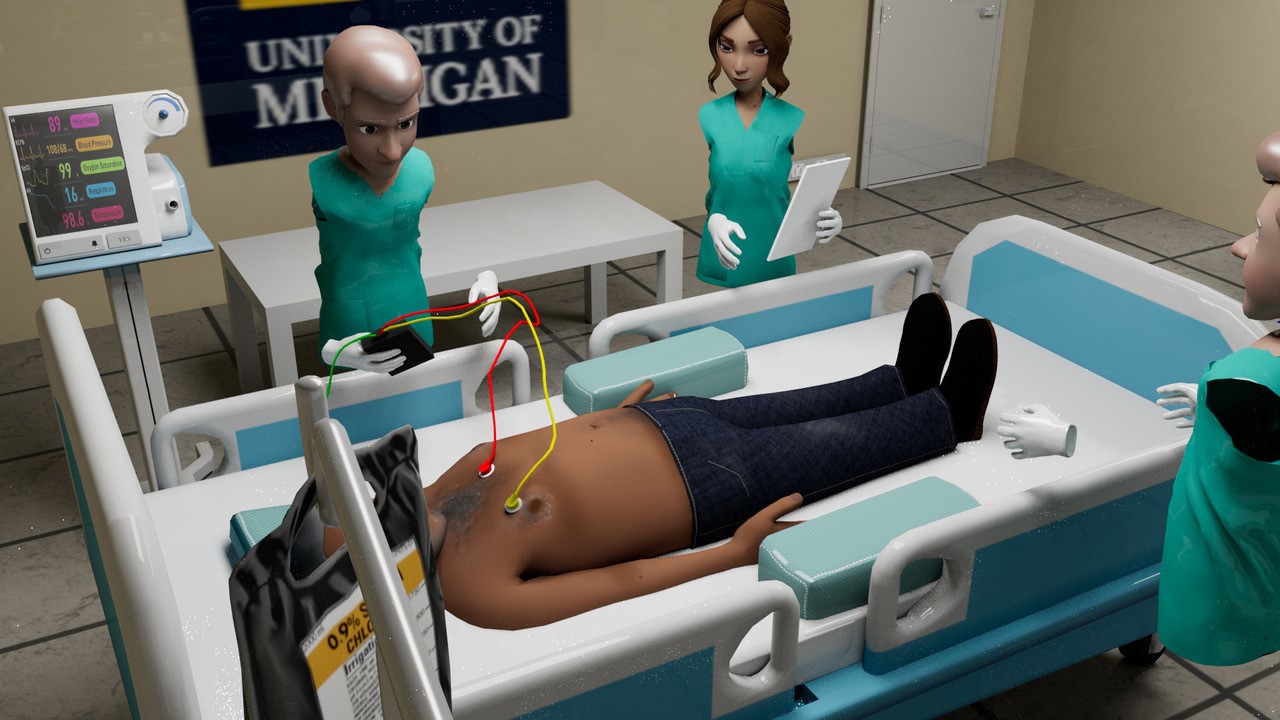
Nelson not only helped Cole select the headsets, but he also helped test the app and the VR systems with users (see figure 2). He ensured they conducted user experience research, including users across various levels of technological literacy, from novices totally new to VR to experienced VR gamers and medical experts. This helped ensure the best end-user experience possible and proper collection and use of sensory data. With the data collected from the live VR project, the team at Michigan Medicine has been able to provide detailed feedback to medical trainees, helping them better understand their experiences and optimal practices during a cardiac arrest. Users receive individualized feedback after completing the training, including feedback on clinical decision-making and a cognitive load score. The team is also using these data to inform the future development of infrastructure for cardiac arrest codes, as well as the creation of new guidelines and policies for these situations.
While this VR project took several years to come to fruition and encountered a few barriers and obstacles, the payoff in training for the low-frequency but high-risk event of a cardiac arrest has the potential to save lives and has helped pave the way for other VR projects at U-M and Michigan Medicine.
Outcomes and Lessons Learned
Plan your VR projects to best utilize the specific benefits VR can provide. One of the reasons this project has been successful is that the planners spent time vetting cardiac arrest training as the type of project that would benefit from the specific capabilities that VR technologies provide. The alternative to a virtual training is far more resource-intensive, the purchase of VR headsets instead of a $150,000 mannequin is an easy choice, and the VR training provides more standardized and better feedback to the users. The VR training has the potential to offer better equity and access as well—users can be training together in different countries, but they all experience the same simulation and aren’t depending on the quality of the instructor to assure a beneficial learning experience. Lastly, cardiac arrest training was best for VR because it doesn’t require as many complex, tactile sensations during the training as other procedures. No one has to practice intubating the patient or putting in an IV in these situations.
Find or create an advocate role between IT and XR business cases. Having an advocate or some kind of bridge role to help work with faculty, staff, and other educators or researchers is well worth the investment. “It takes resources to develop and dedicate this type of position,” said Cole, “but those resources will pay you back tenfold if your institution is serious about supporting XR technologies.” There are many reasons this role can be useful because that person can maintain a view of the bigger picture of XR use at the institution. Researchers and faculty are often siloed in the work they do to plan an XR project, following parallel paths of vendor approval and procurement, contract negotiations, data privacy and security issues, and device use and approval. An XR advocate can help alleviate a lot of undue burdens and common challenges that researchers and faculty face in their development process, helping document application pathways, approved devices, and important staff contacts.
Shop around to find the right developer or vendor for your project. The first step to finding the right vendor or internal developer for your VR project is to conduct a needs assessment and list exactly what will be required. This will enable potential vendors to speak specifically about their ability to meet the needs of any applications or analytics necessary for the project. Cole discovered that no single vendor was able to meet both the app development and attention/cognitive-load data needs, so the team worked with two vendors, one for each aspect of the project. In fact, an initial vendor candidate for app development recommended the attention/cognitive data vendor. “If a vendor can’t provide what you need, your last question of the conversation should be, ‘Who else do you recommend I talk to about this project?,’” said Cole. One other important part of the vetting process was looking at vendors’ previous project successes and outputs instead of listening to potential timelines and promises for the current project. “It always takes longer than what they’ll tell you; almost no one can get one of these projects done in less than 90 days,” added Nelson.
 HP and Intel support the advancement of higher education through the use of emerging technologies. To learn more, visit HP Higher Education. For more information on Intel Technologies, visit Higher Education Technology Resources.
HP and Intel support the advancement of higher education through the use of emerging technologies. To learn more, visit HP Higher Education. For more information on Intel Technologies, visit Higher Education Technology Resources.Where to Learn More
- For more information on the work being done at University of Michigan and Michigan Medicine, feel free to reach out to Michael Cole ([email protected]) or Jeremy Nelson ([email protected]) at University of Michigan.
- Learn more about the HP Reverb G2 Omnicept Edition Headset.
Michael Cole is an Associate Professor and the Co-Director of Interdisciplinary Trauma Team Training at Michigan Medicine.
Jeremy Nelson is the Senior Director of XR, Media Design & Production at the University of Michigan.
Sean Burns is Corporate Researcher at EDUCAUSE.
© 2022 Michael Cole, Jeremy Nelson, and Sean Burns. The text of this work is licensed under a Creative Commons BY 4.0 International License.